Handwritten lecture discussing Anal Fissures in preparation for USMLE Step 2. Will discuss pathophysiology, causes, signs and symptoms, and treatment and management.
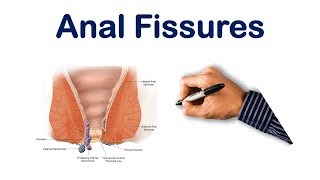
The definition of an anal fissure is a tear in anoderm or distal to the dentate line. This is because this is the are where feel pain. Anterior anal fissue is closer to genitaliia and a posterior anal fissue is on the other side. Posterior anal fissue is more common. Acute is when the anal fissure heals within 6 weeks. Where as chronic is when the fissure is resistant to treatment.
PATHOPHYSIOLOGY and PATHOGENESIS
Stretching of anal mucosa beyond capacity and leads to tear. Spasm pulls on ends of the anal fissures, making it difficult to heal and becomes chronic. Decrease blood flow to certain parts of anus will increase pressue.
CAUSES and ETIOLOGY
Primary causes are due to local trauma. Hard stools due to chronic constipation. Diarrhea specifically prolonged diarrha. Vaginal birth delivery which may cause tear in perineum and final anal sex. Secondary causes is due to previous anal surgery, Crohns disease, Granulomatous TB and sarcoidosis. Malignancy and STDs.
CLINICAL SIGNS AND SYMPTOMS
Parin with defecation is primary symptoms. Bright rectal bleeding on napkin. May also be pruritic. When becomes chronic there is less pain. Upon Examination the fissure will be visible. In acute case the lesion will be red and fresh. Chronic will have raised edges and skin tags will be found. NO DIGITAL EXAM OR PROCTOSCOPY if an anal fissue is seen. This can worsen the anal fissure making it difficult to heal and lead to complications.
TREATMENT and MANAGEMENT
First line treatment is conservative so trying to decrease constipation can allow fissure to heal. So change diet to include more fiber, nitroglycerin and stool softeners and bulk fiber supplements to make defecation easier. Analagesics and creams. Sitz bath can also help with the pain and allow normal bowel movements. Treatments should continue for 1 month. If it doesn't heal than treat for another month. Then this is chronic fissure. Must rule out Crohn's with endoscopy. If it is not Crohn's, then try and reduce spasms with botox, calcium channel blockers, and topical bethanechol for another month. If still not healing then final option is surgery. Lateral internal sphincterectoy and Endoanal-VY advancement flap.
Laternal internal sphincterectomy incisions are made in different areas around the anus and this can release spasm. In the endoanal VY advancement flap. Incisions is made on outside of the anal canal. This can help cover up the fissure. Complications include fetal incontinence. In endoanal VY Advancement flap have 85% success rate.
Category :
Люди и блоги
#anal#fissures#lecture#usmle